We provide you with the best medicine purchasing service
Quickly morph client-centric results through performance based applications. Proactively facilitate professional human capital for cutting-edge.
Download Now
ACUTE MANAGEMENT OF UREA CYCLE DISEASES
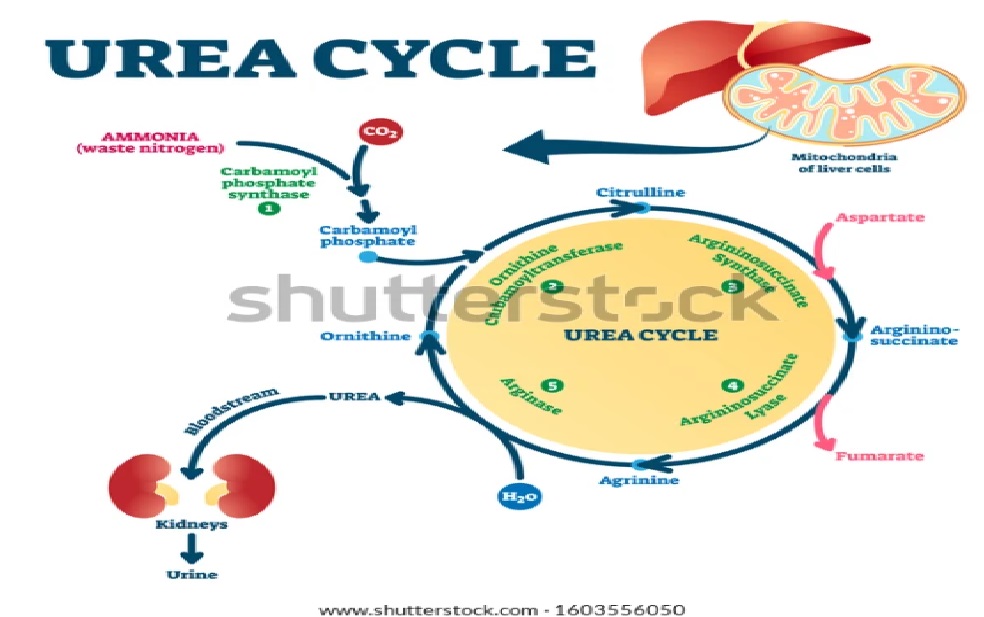
- Such patients easily and frequently decompensate with minor infections, poor oral intake, vomiting or constipation. The patient should be admitted immediately to ER and managed as triage level II.
- Immediate actions which should be accomplished within 1 hour of arrival:
- Basic life support
- Stop all source of protein central and parenteral nutrition.
- Check GlucoChecks.
- Insert an IV line (central and peripheral) and take blood for blood gases, chem 1, Ammonia (NH3), & CBC, blood C/S (peripheral and central if patient has central line). Liver transaminase, Ca, alkaline phosphatase, total protein, albumin, bilirubins, plasma amino acids, urine aminoacids and urine for organic acid (to check for orotic acid).
- Ammonia blood sample should be taken with precaution because of high false positive rate (without tourniquet, in green-top tube, put on ice to the laboratory, separated within 15 minutes of collection and analyzed immediately).
- High caloric intake is the main stay of therapy. Therefore, Start 1 1/2 I.V.F with D10 NS +KCL. (confirm child passing urine before starting KCL)(adjust doses accordingly based on chemistry labs) (Keep GlucoChecks 5-8mmol/L). Consider start insulin if hyperglycemia develop at dose of 0.01-0.05 unit/kg/hour and titrate up until blood glucose controlled.
- The amount of potassium supplement through IV line according to the potassium level result :
- ≥5 = No kcl will be added
- 3.5-4.9= kcl 20 meq/l .If he is on Ammonul : kcl 30 meq/l
- <3.5= 40 meq/l
-
- <2.8 = 0.5 meq/kg kcl as a bolus in prediluted solution D5 w over one hour (should be given centrally and patient should be attached to cardiopulmonary monitor during the infusion) or you can give the required dose of kcl through PO/GT if he can tolerate it. KCL can be given through peripheral line up to 60 meq/l, rate must not exceed 0.125meq/kg/hour.
- Start intralipid 20% at 2-3 g/kg/day to provide additional calories.
- Give a loading dose of ammonia scavengers medications as intravenous infusion over 90 minutes followed by the same maintenance dose divided over 24 hours (see table).
Table: Recommended dosages for medications used in acute management of urea cycle disorders (6, 7):
|
|
Arginine HCl |
Ammonul® (see appendix 3) |
N-carbamylglutamate (Carbaglu®) |
||
|
Kg |
<20 |
>20 |
<20 |
>20 |
Only oral/enteral drug) |
|
Pending diagnosis |
250-400mg/kg. Up to 600mg/kg was recommended |
250-400 mg/kg Up to 600mg/kg was recommended |
250mg/kg
|
5.5gram/m2 |
100mg/kg bolus per NG tube then 25–62.5mg/kg every 6h |
|
NAGS deficiency |
250mg/kg |
250mg/kg |
Not indicated |
Same as above |
|
|
CPS or OTC deficiency |
250mg/kg
|
250mg/kg or 4000mg/m2/day |
250mg/kg Maintenance dose up to 500mg/kg/day |
5.5gram/m2 |
Not indicated |
|
ASL or ASS deficiency |
200-400mg/kg Up to 600mg/kg was recommended |
200-400mg/kg or 12000mg/m2/day |
Same as above |
Not indicated |
|
|
Arginase deficiency |
Not indicated |
Same as above |
Not indicated |
||
Note:
- Arginine HCl, lipid and KCl could be given at peripheral line at the same line (unpublished data from experts).
- Repeat ammonia, blood gases, chem 1 after the loading dose completed.
- Reloading has to be done carefully, in particular during the first 24 h, as cumulative doses of >750 mg/kg/24 h of AMMONUL® have been shown to be associated with development of toxicity (vomiting, lethargy). Reloading only in neonates with severe disorders or those who are undergoing dialysis, and should be spaced at least 6 hours.
- DO NOT DECREASE DEXTROSE RATE or amount and DO NOT STOP calorie delivery in the acute stage for any reason (e.g. medications, addition required fluid bolus, or hyperglycemia) as this can precipitate hypoglycemia and catabolism which will further worsen the patient's condition.
- According to clinical evaluation, empirical antibiotics may be started.
- Ammonia, electrolyte and blood gases need to be followed at regular intervals during this acceleration of management stage. The frequency is dictated by the patient's condition and the speed at which results can be obtained.
- DO NOT STOP other oral chronic medications.
- Proteins should be re-introducing within 24 hours-36 hours of initiation of therapy even if the patients on dialysis.
- Start dialysis if above measures failed to reduce ammonia within4 hours or if initial ammonia is >500 μmol/L.
Frequently asked questions:
- Can we run AMMONUL® on peripheral line?
Yes, on limited based defined as first 24 hours after hyperammonemia crisis.
- Can we run AMMONUL® or arginine with KCL on the same line?
Yes
- Can we run AMMONUL® or arginine with intralipid20% on the same line?
Yes
